
Voltaren Cost
Suitable for: Adults and children aged 14 and over.
24 reviews
Online warfarin dose calculator Warfarin Dose Calculator. Coumadin Adjustment Calculator. This warfarin dosing calculator determines the maintenance dose based on target INR, body surface area and bleeding risk. Warfarin Dosing Calculator. Math is the study of numbers, shapes, and patterns.
We were unable to find any comparative studies of these characteristics conducted here in Brazil. To compare the safety and efficacy of two initial warfarin dosage regimens for anticoagulant treatment. One-hundred and ten consecutive patients of both sexes, with indications for anticoagulation because of venous or arterial thromboembolism, were analyzed prospectively. During the first 3 days of treatment, these patients were given adequate heparin to keep aPTT activated partial thromboplastin time between 1. This prospective cohort was compared with a historical series of patients had been given 10 mg of warfarin on the first 2 days and 5 mg on the third day with adjustments based on INR thereafter. Efficacy, safety and length of hospital stay were similar in both samples. Key words: anticoagulants; warfarin; dose-response drug relationship; thrombosis; treatment outcomes.
Immediate medical attention is required in certain patients, such as in those with bleeding that is severe, does not stop or recurs, or who have other signs or symptoms of concern e. The oral anticoagulants warfarin sodium, acenocoumarol and phenindione, antagonise the effects of vitamin K, and take at least 48 to 72 hours for the anticoagulant effect to develop fully; warfarin sodium is the drug of choice. If an immediate effect is required, unfractionated or low molecular weight heparin must be given concomitantly. These oral anticoagulants should not be used in cerebral artery thrombosis or peripheral artery occlusion as first-line therapy; aspirin is more appropriate for coumadin 8.5 mg of risk in transient ischaemic attacks. The base-line prothrombin time should be determined but the initial dose should not be delayed whilst awaiting the result.
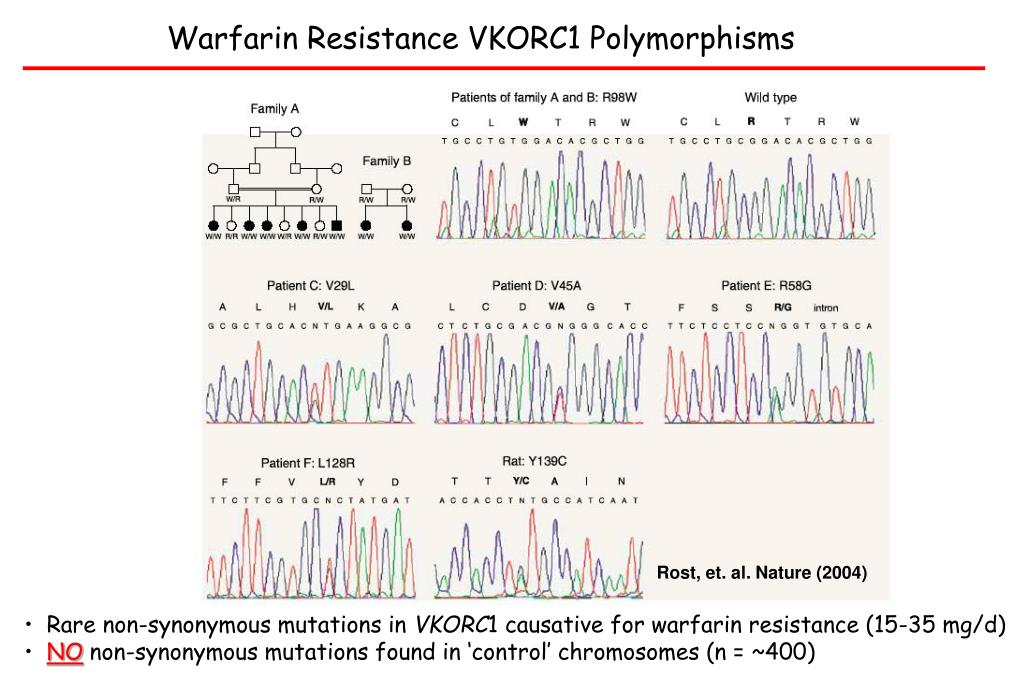
We developed and used an algorithm for estimating the appropriate warfarin dose that is based on both clinical and genetic data from a broad population base. In the validation cohort, the pharmacogenetic algorithm accurately identified larger proportions of patients who required 21 mg of warfarin or less per week and of those who required 49 mg or more per week to achieve the target international normalized ratio than did the clinical algorithm The use of a pharmacogenetic algorithm for estimating the appropriate initial dose of warfarin produces recommendations that are significantly closer to the required stable therapeutic dose than those derived from a clinical algorithm or a fixed-dose approach. The greatest benefits were observed in the Because incorrect doses contribute to a high rate of adverse effects, there is interest in developing improved strategies for determining the appropriate dose. Clinical factors, demographic variables, and variations in two genes — cytochrome P, family 2, subfamily C, polypeptide 9 CYP2C9, coumadin 8.5 mg vitamin K epoxide reductase complex, subunit 1 VKORC1 — contribute significantly to the variability among patients in dose requirements for warfarin.

Warfarin is the most frequently prescribed anticoagulant worldwide. However, warfarin therapy is associated with a high risk of bleeding and thromboembolic events because of a large interindividual dose-response variability. We investigated the effect of genetic and non genetic factors on warfarin dosage in a South Italian population in the attempt to setup an algorithm easily applicable in the clinical practice. A total of patients from Southern Italy affected by cardiovascular diseases were enrolled and their clinical and anamnestic data recorded. The effect of genetic and not genetic factors on warfarin dose variability was tested by multiple linear regression analysis, and an algorithm based on our data was established and then validated by the Jackknife procedure.
Thrombosis Journal volume 6, Article number: 7 Cite this article. Warfarin treatment has a narrow therapeutic range, requiring meticulous monitoring and dosage titration. In the WARIS-II study, comparing three different antithrombotic regimens after coumadin 8.5 mg infarction, warfarin treatment reduced thrombotic events, but was associated with more frequent bleeding than use of acetylsalisylic acid ASA alone. The secondary aim was to relate the genotypes to international normalized ratio INR. Warfarin weekly dose varied between 17 mg and 74 mg among the patients. INR did not vary between genotypes.
Edoxaban Savaysa is a once-daily, oral anticoagulant used to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation. Edoxaban has been compared with warfarin Coumadin for the prevention of stroke and systemic embolism in patients with nonvalvular atrial fibrillation.
Administer dose at the same time every day. May be taken with or without food; food decreases the rate but not the extent of absorption.
Aims In patients recovering from acute coronary syndromes ACS the role of oral anticoagulation and its intensity in addition to aspirin remains controversial. The role of aspirin in the secondary prevention of ischaemic cardiovascular events is universally accepted.
Senna is an herb that comes from several different flowering species of the Cassia plants. The leaves, flowers, and fruits of the senna plant have been used in tea as a laxative or stimulant for centuries. The leaves of the Senna plant are also used in some teas to help relieve constipation or promote weight loss. The most common Cassia senna plants used are the C. Senna is most often used as a laxative, either to relieve constipation or in some cases, to help with weight loss. It is also an ingredient in some conventional over-the-counter laxatives.
As hemodialysis patients were excluded from most clinical DOACs trials, the evidence of their efficacy and safety is lacking in this cohort of patients. Methods and Results: We included five studies with a total of 34, patients in our meta-analysis. The outcomes were major bleeding, ischemic stroke, systemic embolization, hemorrhagic stroke, gastrointestinal bleeding, minor bleeding, and death. Of these patients, 31, However, there were higher rates of systemic embolization, minor bleeding, and coumadin 8.5 mg events in patients who received DOACs than in the warfarin group 3.
Suitable for: Adults and children aged 14 and over.

Use cautioin in obstructive genitourinary tract disease, asthma, pyloric or duodenal obstruction, prostatic hyperplasia, narrow angle glaucoma.

Zyloprim Metoclopramide Ranitidine Cytotec.